Healthcare & Clinical Research Software Trends in 2026:
What Engineering Leaders
Must Build Now

Healthcare & Clinical Research Software Trends 2026
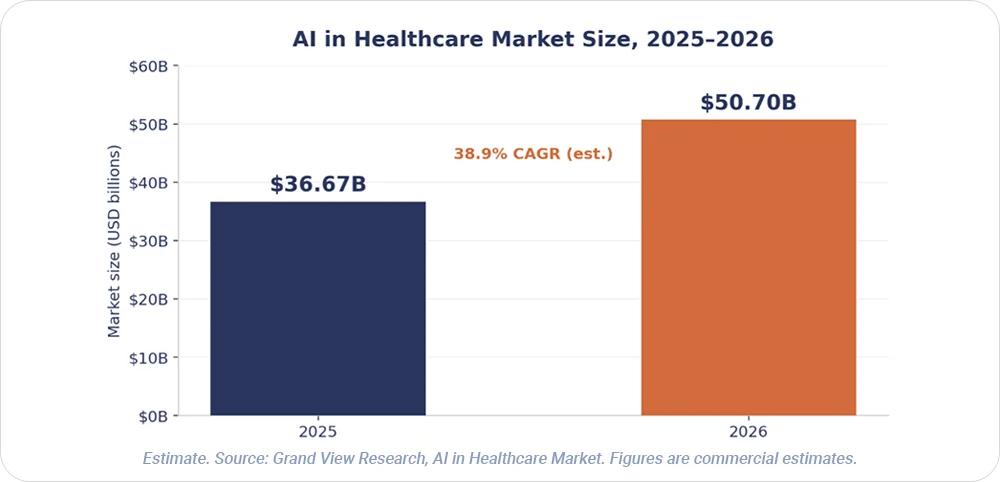
The digital transformation in healthcare market sits at an estimated $98.5 billion in 2026 and is projected to reach $381.5 billion by 2036 at a 14.5% CAGR, per Future Market Insights. Grand View Research separately estimates the AI in healthcare market grew from $36.67 billion in 2025 to $50.70 billion in 2026, a 38.9% CAGR through 2033. Both are commercial estimates. Software accounts for approximately 75% of the digital transformation in healthcare market, per a separate Fact.MR model. The companies that will lead in 2027 are making architecture decisions now.
Regulatory activity has accelerated alongside the spend. The FDA's AI/ML-enabled medical device list has grown substantially through 2025 and 2026 across radiology and other specialties — engineering leaders should read the FDA list directly and record the access date when citing a count. Six software trends now separate teams that ship safely in regulated environments from teams that stall.
Softwarium is a US-headquartered software engineering and IT staff augmentation company with an EU-based engineering delivery network and 25+ years building custom digital products for healthcare software companies, pharmaceutical and life science organisations, and clinical research technology vendors.
TREND 1: Ambient AI Has Become Operational Infrastructure in Healthcare Software
Physicians have moved AI from pilot to daily practice. The AMA's 2026 Physician Survey on Augmented Intelligence found that 81% of physicians used AI in their practices, compared with 38% in 2023. That figure spans administrative, documentation, research, and clinical applications — it does not mean 81% use diagnostic AI. Adoption now concentrates on workflow tasks such as research summarisation and clinical documentation.
The burnout signal is concrete but bounded. In a 30-day multicentre quality-improvement study (PubMed 41037268), the proportion of participating clinicians reporting burnout declined from 51.9% to 38.8% after ambient AI scribe deployment. The result reflects that study design and timeframe; it does not generalise to all health systems or all AI tools.
Engineering implication
Ambient and decision-support features depend on real-time ML inference pipelines, HL7 FHIR R4 EHR integration with Epic and Oracle Cerner, and NLP/NLU for clinical documentation (Azure OpenAI, Amazon Comprehend Medical). SMART on FHIR architecture governs authorisation. Where an AI tool crosses the clinical decision threshold, FDA SaMD classification awareness moves from optional to mandatory.
AI and ML engineering for clinical data environments is where most healthcare software product teams hit their first regulated-data wall.
TREND 2: FHIR APIs Have Become Core Infrastructure for US Healthcare Products
Interoperability requirements now shape product roadmaps for healthcare software companies. CMS interoperability rules require specified payer categories — Medicare Advantage organisations, state Medicaid and CHIP programmes, managed-care entities, and QHP issuers on federally facilitated exchanges — to implement FHIR-based APIs, with major API provisions taking effect primarily in January 2027 under CMS-0057-F. ONC applies separate FHIR requirements through the Health IT Certification Program; since January 2023, users of certified EHR technology have been required to have standardised FHIR APIs available, per healthit.gov. These are two distinct frameworks covering different parties — not one universal provider mandate.
Engineering implication
Delivery centres on FHIR R4 server and client development, SMART on FHIR OAuth2, and HL7 v2-to-FHIR mapping pipelines, with SNOMED CT, LOINC, and ICD-10 terminology services underneath. EHR integration testing runs against the Epic Sandbox and the Cerner FHIR API. For clinical research technology vendors, FHIR is converging with CDISC standards to enable EHR-to-trial data flow — a concrete engineering opportunity, not a future one.

TREND 3: Decentralised Trial Capability Has Become a Standard Platform Evaluation Criterion
Clinical research technology vendors now compete on decentralised trial support. The regulatory anchor is the FDA's September 2024 final guidance on conducting clinical trials with decentralised elements. ICH E6(R3) provides the current international GCP framework, implemented through participating regulatory authorities; the FDA issued its final E6(R3) guidance in September 2025. Vendor commentary from sources such as RealTime eClinical and Clinical Trials Arena reads as attributed industry opinion, not established market fact.
Scope discipline matters here. Clinical-trial systems that create, maintain, or submit FDA-regulated electronic records require a documented 21 CFR Part 11 applicability assessment — Part 11 does not attach automatically to every eClinical system. EU Annex 11 applies where computerised systems support GMP-regulated activities under EudraLex Volume 4, not to every decentralised clinical trial platform.
Engineering implication
Decentralised trials require eConsent, remote monitoring integration, ePRO mobile, and IRT systems connecting to EDC, CTMS, and analytics. The build list runs to FHIR-integrated EDC/eClinical platforms, eConsent and ePRO mobile architecture, CDISC ODM/SDTM data pipelines, validated audit trail design, and cloud-native eClinical microservices.
Healthcare technology companies partnering with Softwarium gain access to distributed engineers with experience in HIPAA-compliant data architecture, HL7 FHIR API integration, AI and ML engineering for clinical data environments, and quality assurance for regulated healthcare and clinical research software systems.
Scaling Your Healthcare or Clinical Research Platform?
TREND 4: Remote Patient Monitoring Has Expanded From Post-Pandemic Supplement to Reimbursed Clinical Channel
Reimbursement has changed the engineering stakes for connected health. The mHealth app market reached an estimated $46.16 billion in 2026, growing at 13.5% year-on-year (market-sizing context). CMS introduced three HCPCS codes for qualifying digital mental-health treatment devices effective January 2025; these codes apply to qualifying devices used alongside a behavioural therapy plan, per the CMS behavioural health integration document. The reimbursement step is specific — it is not evidence that RPM broadly became primary-care infrastructure.
Software functions that meet the medical-device definition require a regulatory-pathway assessment based on intended use, risk, classification, and applicable FDA guidance, per FDA SaMD guidance. The determination depends on multiple factors and does not reduce to a single 510(k)-or-De Novo choice.
Engineering implication
RPM platforms run on IoT sensor data pipelines and real-time streaming architecture (Azure Event Hubs, Kafka), HL7 FHIR Device resources, and HIPAA-compliant data architecture, with SaMD classification awareness and mobile-first clinical UX shaping the front end.
TREND 5: Healthcare Cybersecurity Has Become a Patient Safety Engineering Problem
Breach data frames cybersecurity as an engineering responsibility, not an IT afterthought. As of June 2026, the HHS OCR portal listed 772 breaches reported for 2025 affecting approximately 139.7 million individuals — OCR records continue to change as incidents are added or amended (analysis via HIPAA Journal; primary data at the HHS OCR portal). The average cost of a healthcare data breach is $7.42 million — the highest among studied industries for the 14th consecutive year, per IBM's 2025 Cost of a Data Breach report.
Claroty reported known exploited vulnerabilities in 99% of healthcare organisations included in its analysed dataset — a dataset-scoped finding, not a census of all hospitals. The healthcare sector accounted for approximately 22% of all disclosed attacks in 2025, with ransomware remaining the top threat, per the Health-ISAC 2025 Annual Threat Report. For medical device cybersecurity, IEEE/UL 2933-2024 addresses clinical IoT data and device interoperability under TIPPSS principles; premarket device cybersecurity submissions fall under FDA's February 2026 guidance on quality management system considerations.
Engineering implication
The controls list runs to zero-trust network architecture, HIPAA Security Rule-compliant infrastructure, BAA-aware vendor integration, encrypted PHI in transit and at rest, and healthcare-specific incident response planning built into the delivery pipeline.
TREND 6: AI Is Reshaping the Engineering Infrastructure Behind Drug Discovery and Clinical Research
Regulators have absorbed years of AI submissions. The FDA has reviewed more than 500 drug and biological product submissions containing AI components between 2016 and 2023, per its framework press release. In January 2025 the FDA published a draft guidance proposing a risk-based credibility framework for AI models used to support regulatory decisions; it remains draft guidance as of June 2026. The FDA and EMA jointly published good AI practice principles in January 2026, a marker of regulatory maturation.
A 2025 Nature Medicine randomised Phase 2a study of rentosertib marked a clinical milestone for AI-enabled target identification and molecule design. The study is a Phase 2a signal with limitations including short duration and withdrawals. On success rates, a 2024 analysis of a limited sample of AI-discovered molecules reported Phase I success rates of 80–90%; Phase II performance in the same limited sample was approximately 40%, close to historical averages. A total count of AI-originated drugs in trials is not reported here, because no named registry with defined inclusion criteria and search date supports one.
Engineering implication
Drug discovery and clinical research data platforms depend on multi-modal biomedical data platforms, molecular ML model pipelines, CDISC SDTM/ADaM data transformation, cloud-native data lakes for regulated research, and regulatory submission data packaging.
What Engineering Leaders Must Build Now
Healthcare and clinical research software teams need engineering partners who understand the regulatory context, not just the technology stack. Domain-aware engineering closes the gap between shipping fast and shipping safely in a regulated environment, and it is the difference between an architecture that scales and one that becomes a compliance liability. The digital transformation in the healthcare market rewards teams that build for HIPAA, FHIR, GCP, and SaMD scope from the first commit instead of retrofitting them later.
Build With a Partner That Knows
the Regulatory Context
Softwarium builds and scales engineering teams for healthcare software and clinical research technology companies.
Prefer the dedicated development team model? See Softwarium services.
Book time with Anna Moskalets, Head of Sales EMEA: Calendly.


